
In February 2022, Russia attacked Ukraine in what was only the start of an ongoing war. Millions of Ukrainians fled the country, with more than a half million passing through Moldova, spending a few days before transiting to other countries. During the summer of 2022, around 80,000 remained in Moldova.
Leslie deployed to Moldova for three months to work on health programming for Ukrainian refugees in the country, as well as to support internally displaced people (IDPs) who were remaining in the Odessa Oblast in Ukraine.
Meeting the medical needs of refugees in Moldova looked very different than typical refugee medical needs, which required creative programming to meet the objectives. Most refugee situations occur in areas of the globe where there is already limited medical care, and an influx of refugees overwhelms the system. Foreign aid agencies often bring in field hospitals and foreign staff to be able to meet these needs.
In Moldova, however, the medical system was well-established and could absorb the influx of refugees. Furthermore, the disease care looked different: while most refugee situations require acute medical care associated with fleeing on foot from violence, most of the Ukrainian refugees needed help with chronic medical conditions, such as diabetes or heart disease. They needed help with continuing to receive the medications and treatment they had ongoing in Ukraine.
In Moldova, they could visit clinics and hospitals for free, but medications were not covered. Furthermore, Moldova experienced strains in their supply chain, as many medications and basic hospital supplies came from Russia or Central Asia, and those supply chains broke during the war.
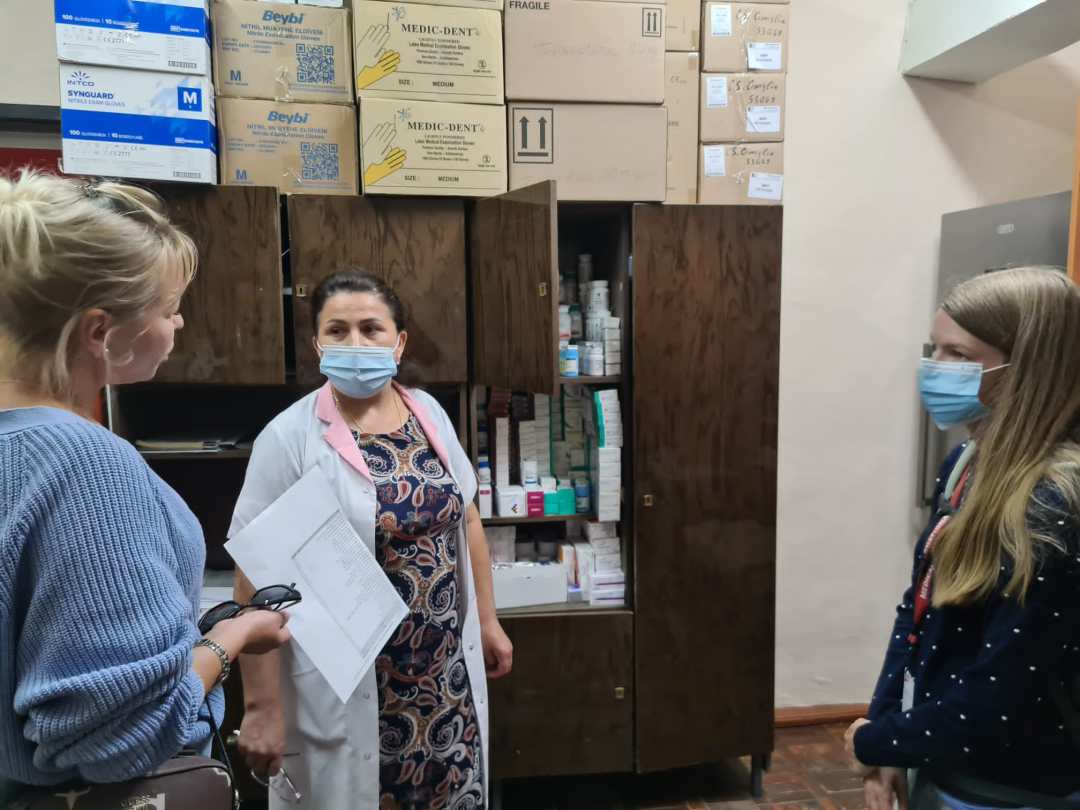
The programming was designed around a health system strengthening approach. It aimed to relieve these supply chain issues by using other sources of medications, keeping hospitals and clinics stocked on supplies. Furthermore, clinics and hospitals with nearby large Ukrainian refugee populations were supplied with a special pharmacy of medications for refugees. These medications were free for refugees to ease the burden of cost and increase healthcare access for them.
The program also funded transportation to clinics and hospitals for refugees who were staying at refugee accommodation centers (RACs), in order to maintain access with as little barrier as possible. RACs also were supplied with basic first aid kits and medical supplies to be able to help refugees on site.

Leslie also oversaw and approved of unique cases of medication needs that were beyond the list of essential medications supplies to the hospitals. In one case, a Ukrainian Roma had been receiving chemotherapy for leukemia when the war broke out. As we was 17 at the time, for a brief period he could travel back to Ukraine to get his chemotherapy. But after he turned 18, he had to make a difficult decision: return to Ukraine for treatment and not be able to leave again, as men of military age could not leave the country, or stay in the safety of Moldova and not have access to chemotherapy. Leslie and the Moldavian team were able to source the same drug in Moldova and pay for it through the medical programming, as well as pay for the routine laboratory visits he needed for bloodwork during the treatment.
Finally, the programming also included training on Psychological First Aid (PFA). Recognizing that it wasn’t just physical health needs that needed met, the team incorporated training for those who would be in regular contact with refugees, such as staff working at RACs and staff at the medical centers. PFA teaches people how to talk with those who have experienced trauma and help guide them in the direction they need for more care, whether physical, emotional, mental, or spiritual.
Much of this programming was also mirrored in the Odessa Oblast, where IDPs needed much of the same care: free medications after being displaced from where they lived, and PFA training for those who helped IDPs.
All this programming reflects the need for adaptability to the local context. The model that works well in some contexts will not function in others. Careful analysis of the situation, done through needs assessments, action research, and involvement with community members and local stakeholders will help gear a program to better suit the real needs of the population.
